
5 Weeks Gestation: What Should I See?
When a patient presents for an ultrasound at five weeks of gestation, we are often unsure of what we will be able to see on the scan. Many times, I warn my patients ahead of time to not get discouraged if we don’t yet see the fetal pole with a heartbeat. Sometimes, it is just a little too early.
Our focus should be documenting that the pregnancy is in fact intrauterine, however, much of what we see can depend upon the patient’s beta-hCG. By five weeks gestation, we are likely to see at least a gestational sac. With transvaginal ultrasound, an intrauterine pregnancy can usually be seen with a beta-hCG of 1,000-1,500 IU/L. Sometimes we can also see a yolk sac and by about 5w5d, we may even see a fetal pole with cardiac motion. The fetal pole can be compared to a grain of rice, as they appear very similar in size and shape. We do not see limb buds at this early gestation, and it can be difficult to determine which end is the crown and which end is the rump. There also will not be any voluntary movement of the fetal pole noted. It is not uncommon for the fetal heart rate to be lower than usual right around the 5–6-week gestation period, from 100-120 bpm can be normal. Remember to measure the fetal heart rate with M-mode in the first trimester!
As with any first-trimester scan, you want to perform sweeps through the entire pelvis (uterus and adnexa) to evaluate for the five A’s – assess, alive, alone, age, and anomalies. Early pregnancies are best evaluated with the transvaginal probe.
In the case study below, you will see the progression of a pregnancy from around 5 weeks to just over 6 weeks.
Case Study
Patient presented as a 36-year-old G5P1031 with a positive pregnancy test. LMP is noted to be March 27. The patient has had 3 prior SABs, so she requested a beta-hCG be drawn. On May 8, the beta was 1238 IU/L. With this beta, we should be able to confirm an intrauterine pregnancy with transvaginal ultrasound.
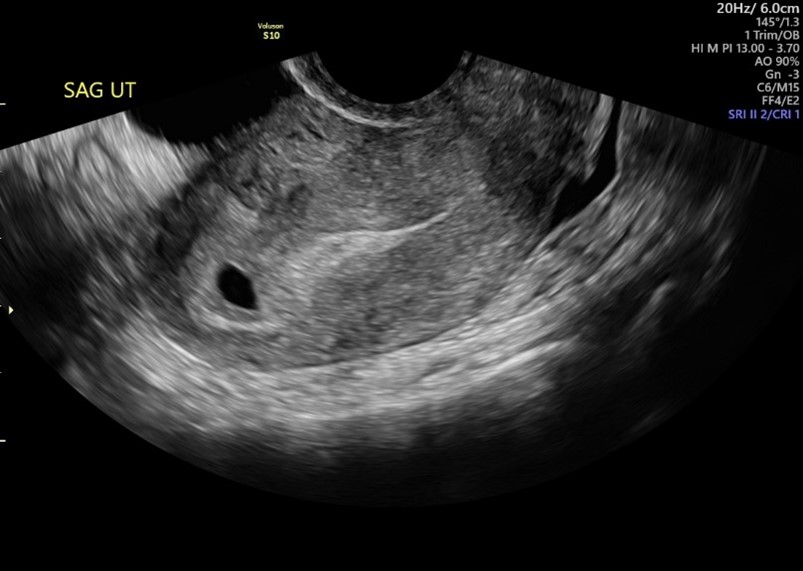
Transvaginal ultrasound performed on May 9 demonstrates an anteverted uterus with a single gestational sac seen. A double decidual sign is noted. The double decidual sign are the two concentric rings surrounding the anechoic gestational sac. This is important to differentiate between a gestational sac and a pseudosac before seeing a yolk sac or an embryo.
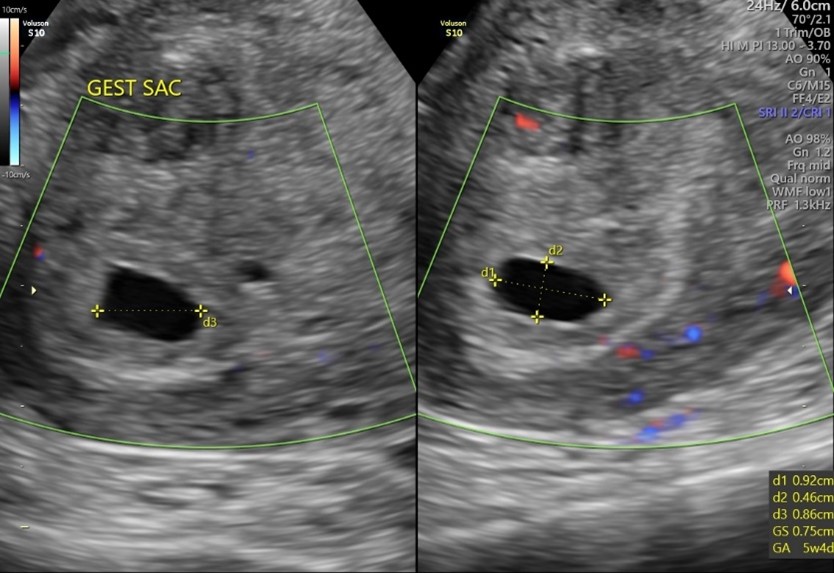
Measuring Mean Sac Diameter
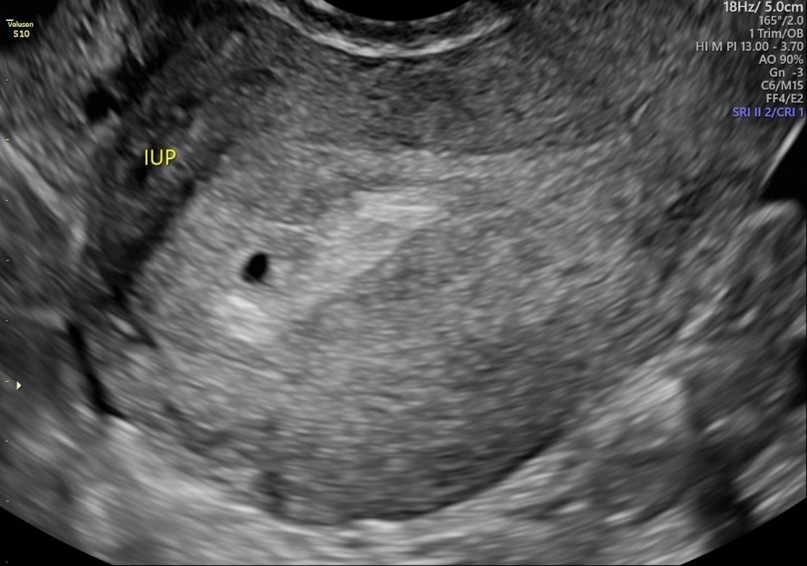

The mean sac diameter measured .39 cm or 5w1d -7 days different from her LMP date.
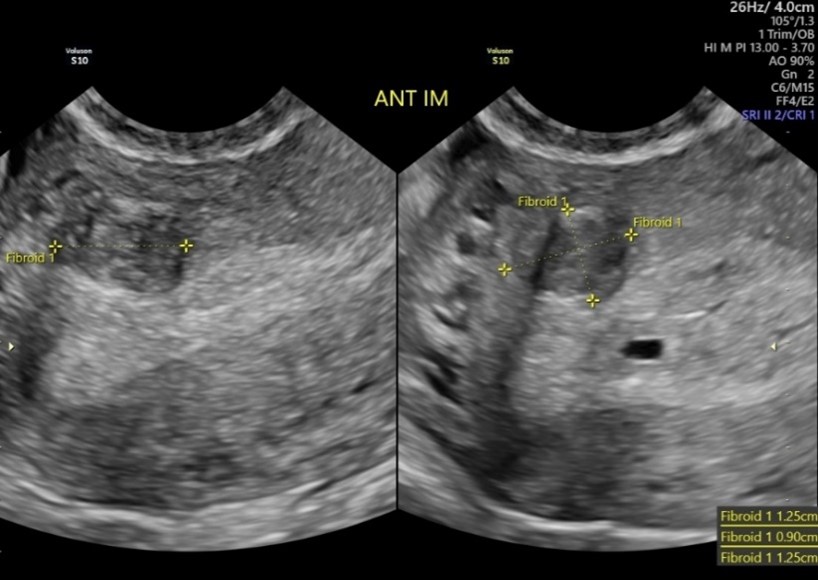
Incidentally, at this scan, an anterior and intramural fibroid is seen as pictured above.
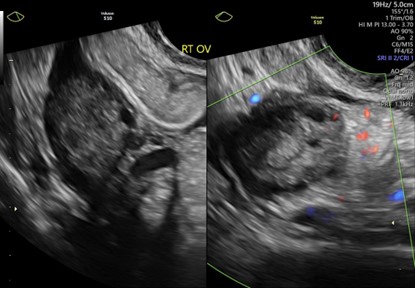
Assessing Adnexa
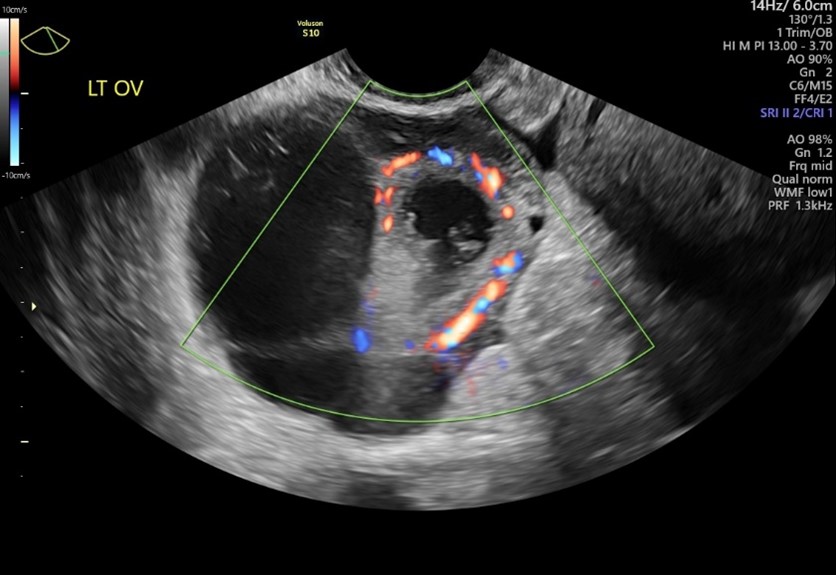
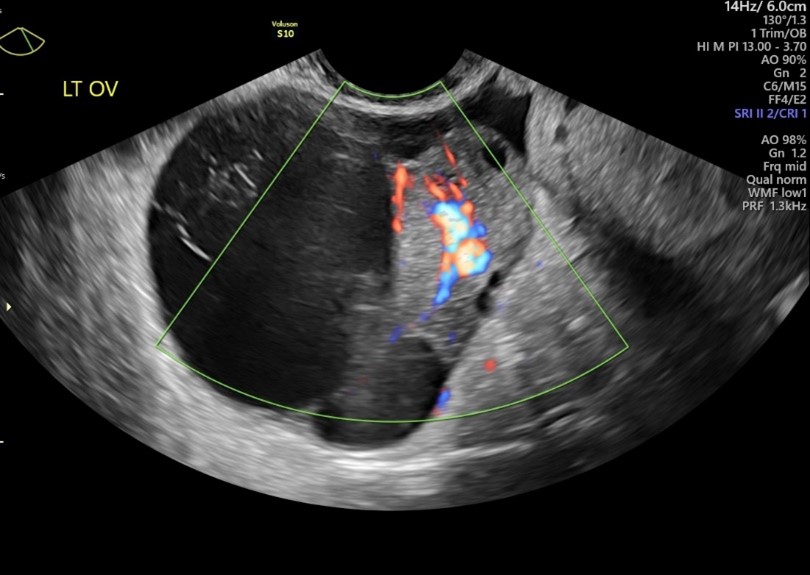
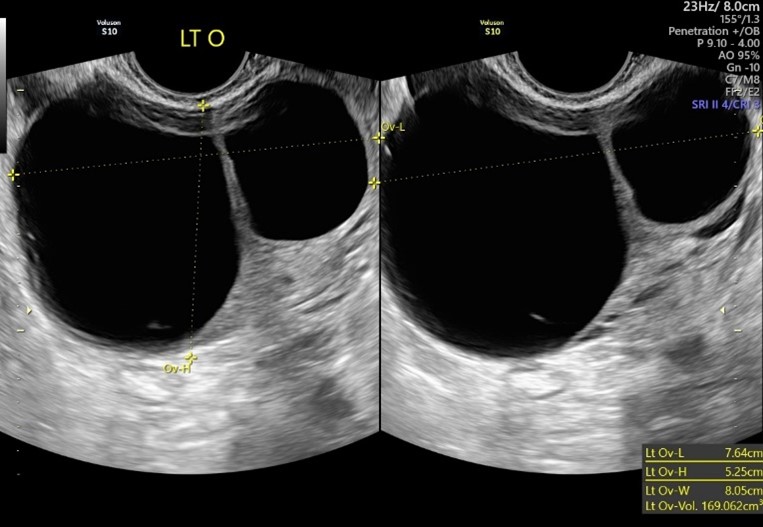
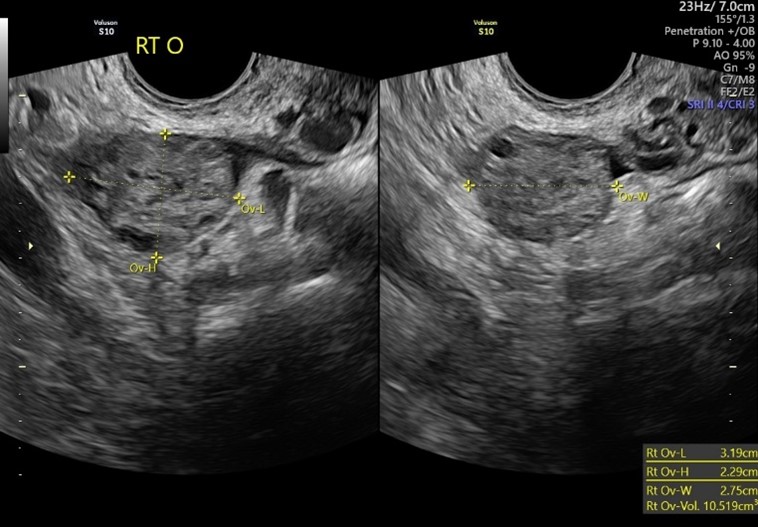
Also, a large multi-locular left ovarian cyst is seen with some solid components (see below). Vascular flow is noted within with the use of color Doppler.
The right ovary was also evaluated for comparison, and it appears normal, as seen below.
The beta-hCG was repeated on May 10 and was reported as 3251 IU/L, which is a normal and expected increase.
First Follow-Up Exam
The patient returned for a follow-up scan on May 13, where the intrauterine gestational sac now measured 0.75cm or 5w4d was seen. No yolk sac or fetal pole seen. The gestational sac showed appropriate growth between scans.
Not pictured is the stable left ovarian cyst and intramural fibroid, as there was no change between the two scans.
Second Follow-Up Exam
The patient returned a week later, on May 17. A yolk sac and fetal pole were both seen, as pictured below. 3 CRLs were obtained and averaged at 5w5d.
Once a fetal pole is present, we no longer measure the gestational sac.
The EDD is established at 1.12.25 since we have a fetal pole to measure, and there is greater than a 5-day difference between the average CRL and the patient’s LMP. No cardiac motion was detected on this ultrasound. Although the measurement of the CRL at 2.2-2.5mm is too small to diagnose pregnancy failure.


Again, the intramural fibroid and left ovarian cyst were noted to be stable in size and appearance.
Third Follow Up Exam
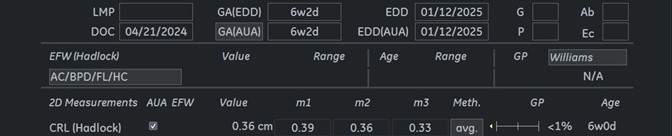
The patient returned on May 21 and a fetal pole measuring an average of 6w2d was noted with positive cardiac motion detected. Appropriate growth was seen between the last two scans. The cardiac motion appears normal on several cine clips; however, the sonographer was unable to obtain an accurate m-mode measurement simply due to the small size of the fetal pole and exam limitations, like maternal body habitus.


The fibroid is stable, and the left ovarian cyst appears improved. No solid components and no vascular flow within seen at this time. Right ovary is normal as pictured below.
Below is our report page that shows the fetal pole measures on track or consistent with the earliest ultrasound performed. Due to the patient’s history of SAB x 3, the patient will be monitored more closely and will likely have another ultrasound to confirm appropriate growth and FHR around 9-10 weeks gestation.
As we discussed, by 5 weeks or with a beta-hCG of 1,000-1,500 IU/L, we should see a gestational sac in the uterus. The double decidual sign is a positive sign that what you are seeing is a gestational sac and not a pseudo sac, sometimes seen with ectopic pregnancy. By about 5w5d-6w0d, we should visualize a yolk sac and a fetal pole with + cardiac motion. Proceed with caution and follow up in 7-10 days if those are not seen before diagnosing pregnancy failure. There are exceptions to every rule, and sometimes, exam limitations can prevent us from seeing the entire picture at such an early gestational age.
You can learn more here: https://sonosession.com/product/introduction-to-ob-gyn-ultrasound-2/