
Placental Abruption is a rare, but serious, condition of pregnancy. It is defined as the premature separation of the placenta from the uterus. Urgent medical attention is always recommended, as placental abruption can be life threatening if not treated. It is reported that there are fewer than 20,000 cases per year in the United States.
Placental abruption may be caused by abdominal trauma or injury, sudden loss of amniotic fluid, high blood pressure, smoking, substance abuse, multiples, prior pregnancy with placental abruption, and pregnancies over 40.
Placental abruption can be seen on ultrasound but is also very much a “full picture” scenario. The clinical signs and symptoms that the patient presents with are just as important as the ultrasound findings. Symptoms may include vaginal bleeding, abdominal pain, symptoms of early labor and fetal distress.
In the following case study, you will see how with ultrasound and proper clinical correlation, we were able to diagnose placental abruption and treat immediately.
CASE STUDY
The patient presented as a 29-year-old G1 at 35w6d for a BPP with umbilical artery Dopplers due to a recent diagnosis of fetal growth restriction just the week prior. The patient contacted our office that morning with complaints of vaginal bleeding and abdominal pain, and she was instructed to keep her appointments as scheduled.
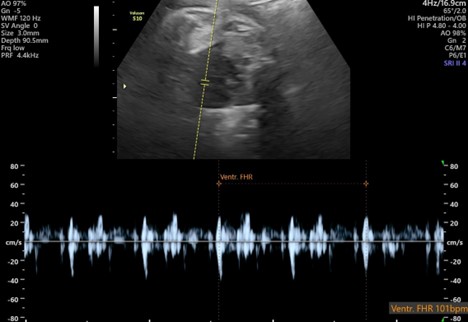
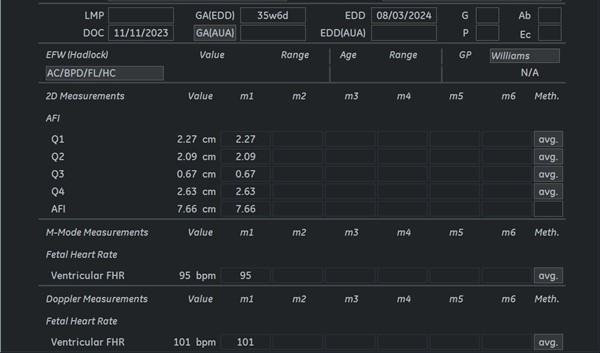
Upon beginning the exam, the fetal heart rate was noted to be low at 101bpm. Normal range is 120-160bpm.
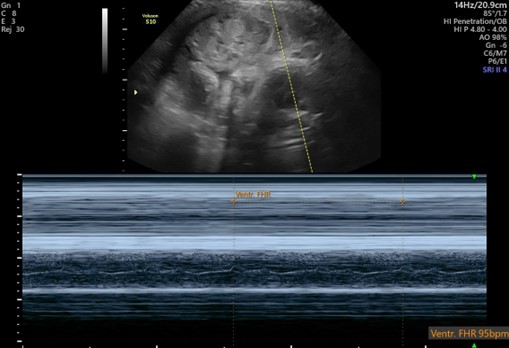
The repeat M-Mode tracing of the heart rate demonstrated 95bpm.
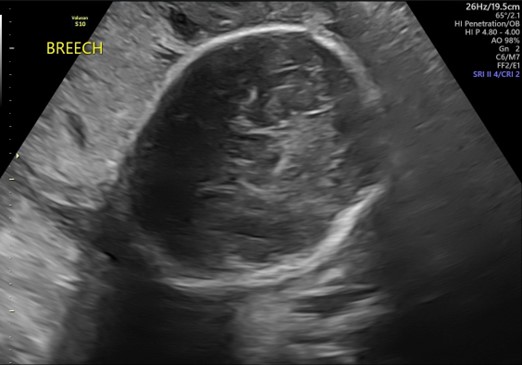
The baby was noted to be in breech presentation – head up and bottom down.
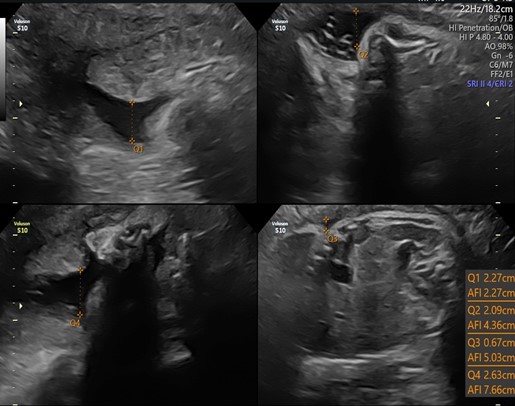
The amniotic fluid measured within the lower limits of normal at 7.66cm.
There is an anterior fundal placenta.
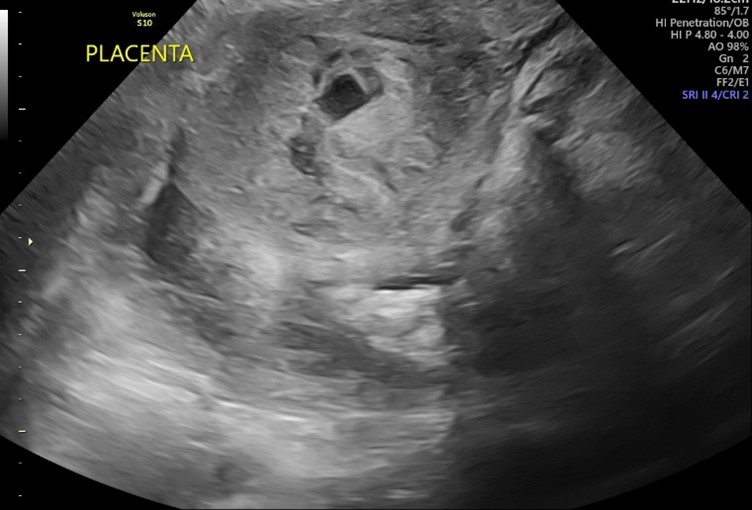
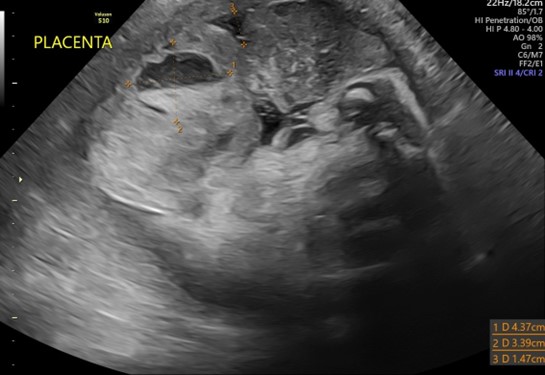
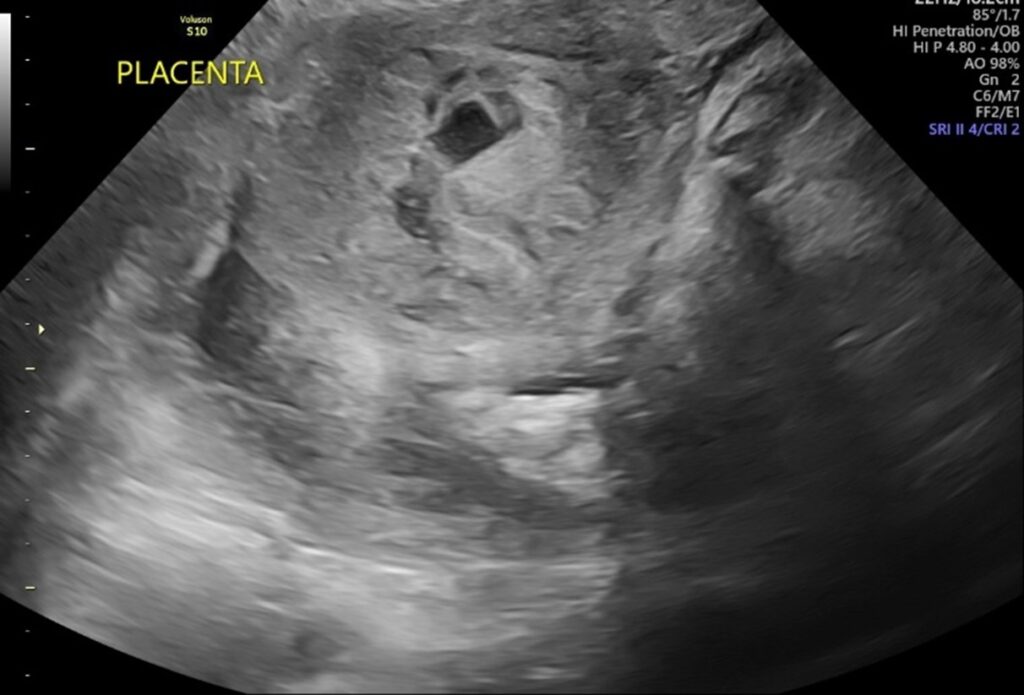
Notice the large 4.4cm hematoma appearing structure that is measured here as well as the 1.5cm separation from the placental wall:
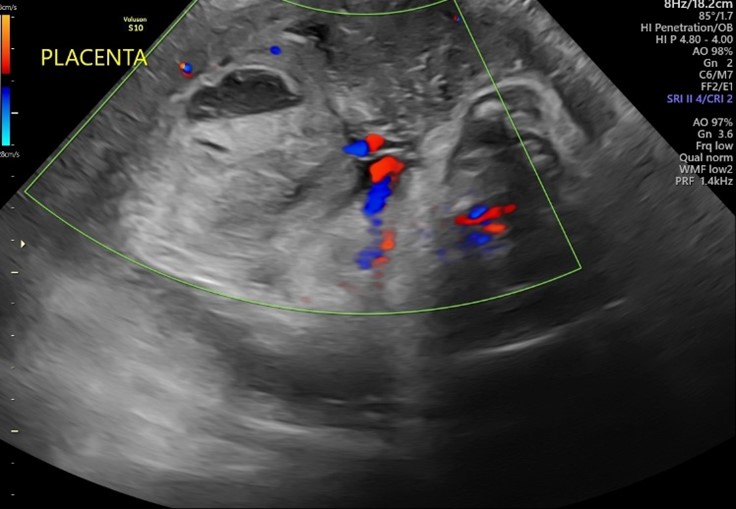
There is also a large pool of blood noted in the posterior aspect of the image:
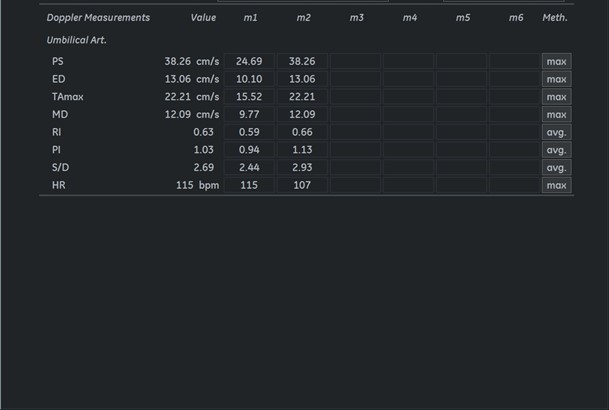
Umbilical artery Dopplers were performed due to fetal growth restriction. Both were normal.
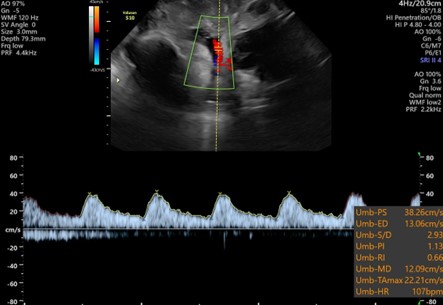
The report shows the amniotic fluid volume, the low fetal heart rate, and the normal Dopplers.
Due to the very low fetal heart, the appearance of the placenta, and the patient’s symptoms of bleeding and abdominal pain, the diagnosis of placental abruption was highly likely. The BPP was suspended, and the patient was sent to L&D. An emergency c-section was performed within 45 minutes of sending the patient over. Placental abruption was confirmed as the uterus was filled with blood. The baby weighed 4lbs 12oz and had Apgar scores of 7 and 9. The patient and baby are doing well now. Other related topic here